


We need adaptable and accessible communication strategies to address vaccine hesitancy and vaccine indifference in the most vulnerable sections of our society.
While the COVID-19 virus has touched every corner of the globe, its impact on the ground has been far from uniform. In developing countries, where over 1 billion people live in slums, factors such as population density and poverty prohibit pandemic-safe behaviours like physical distancing and work-from-home.
In developing countries, the socio-economic effects of the pandemic will be long-lasting, as it has reversed decades of progress in poverty eradication and food security. In India, this is reflected by the 230 million people who have been pushed into extreme poverty since the onset of the pandemic.
While several pandemic-related challenges, like flattening the curve, have been more difficult in developing nations due to factors like weaker, less resilient infrastructure and healthcare systems, there is one issue that developing and developed nations alike are struggling to overcome: crossing the threshold to achieve complete immunisation against the virus.
While each country faces its own unique set of challenges in procuring and administering COVID-19 vaccines, an overarching hurdle is the need to combat vaccine hesitancy.
The coronavirus has triggered two parallel pandemics: a virus spreading across the globe and an info-demic, spreading across mass media. From innocently misleading to intentionally deceiving, misinformation and disinformation about vaccines are rampant.
India is no exception to this phenomenon. Even though India has seen great successes in the past with nationwide vaccination campaigns to eradicate polio and measles, the rapid spread of unchecked information due to the advent of digital media, has increasingly propagated false information, threatening public health.
At the root of vaccine-related misinformation lies not only mistrust and fear, but also legitimate questions and doubts. Vaccines are efficient public health tools to reduce disease burden, yet people continue to be “vaccine hesitant”. Another barrier to vaccine uptake is “vaccine indifference” — where people, dealing with the compounded effects of the pandemic on their livelihood, education, and quality of life, don’t rank getting vaccinated high in their list of priorities.
Crafting Communication
We need tailored communication strategies to address the different barriers to vaccine uptake in India. Studies have shown that simply correcting myths about vaccines not only fails to improve intention to vaccinate, but also may backfire and decrease intention to vaccinate.
By understanding the motivation behind the hesitancy, we can create communication approaches that speak to that motivation, match the reality of the receiver and do more than simply replacing rumors with ‘facts’. We need to ensure that there are accessible and adaptable communication channels which allow communities to ask questions and receive information about the vaccine and the vaccination process. The effectiveness of this process requires patience, resources and people.
Samhita’s response to the vaccine uptake challenges has been to focus on information communication in tandem with increased accessibility. Evidence-based educational and training materials from field practitioners, medical and public health agencies, and clinicians are made available to NGOs and organizations working on the ground. For example, in the district of Satara, Samhita has helped build awareness and conduct surveillance surveys to understand and record changes in COVID appropriate behaviour, vaccine hesitancy, and information gaps about home-based COVID care, among frontline health workers, ASHA workers, Anganwadi workers, etc.

Leaving No One Behind
Immunisation is one of humanity’s greatest achievements, but a large portion of the world’s population are still not benefiting from it because they cannot easily access and avail the vaccines. Ensuring public health is the first step to building just and sustainable societies and economies — in a pandemic, vaccines are a highly cost-effective way to do that.
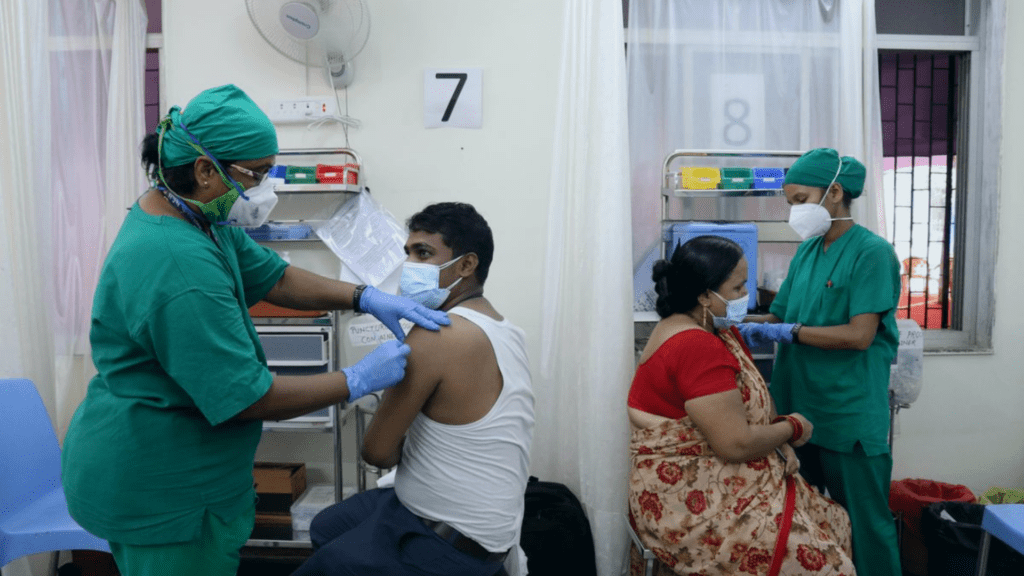
To help vaccinate daily wage workers and marginalised communities who are likely to get left out of the current vaccination program, Samhita has designed the following interventions to navigate their COVID related challenges and doubts:
- Facilitation and administration of the vaccine in large proportions. With the collaborative support of private organisations, large cohorts could be covered in a short span of time.
- Identification, registration and mobilisation of beneficiaries at scale.
- Inoculation process, post inoculation monitoring; providing a robust technology platform to manage the programme and monitor the vaccinations.
- Community-wide immunisation drives to inoculate at-risk vulnerable communities who have either very little or no awareness about the vaccination programme.
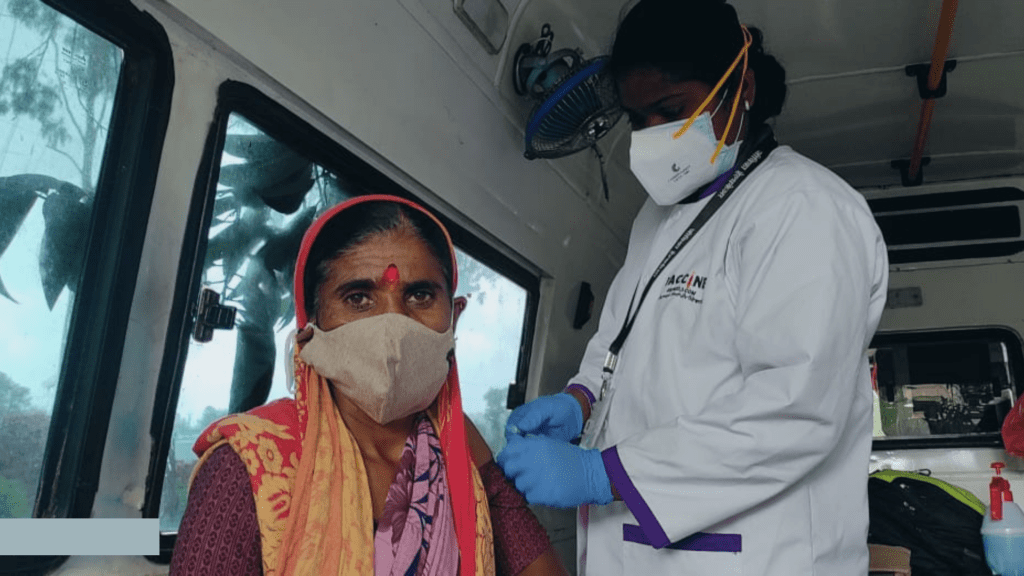
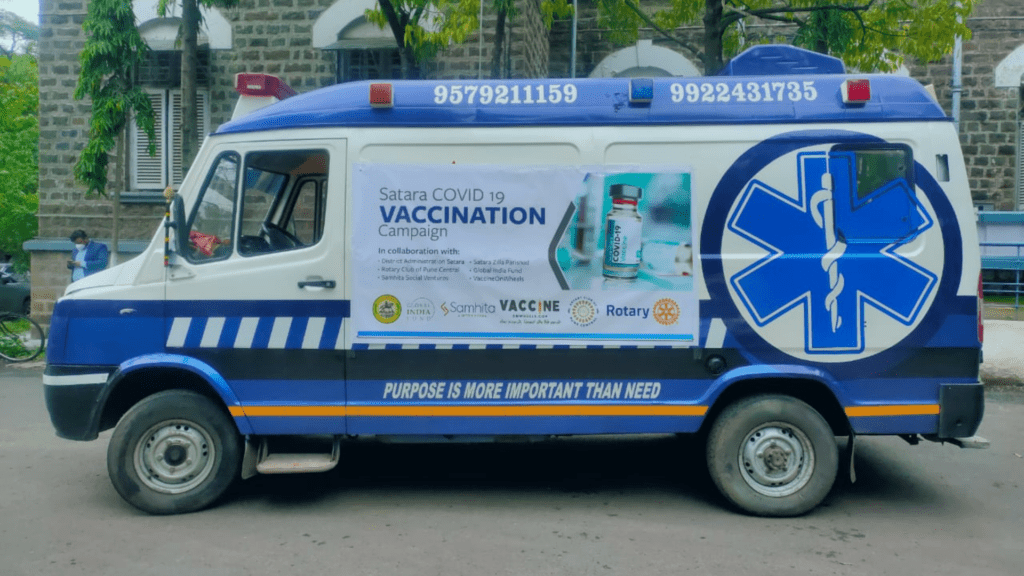
- Mobile vaccination through mobile vans for reaching out to communities in rural and tribal areas.
Through these interventions, one of the most prominent transformations observed was significantly higher confidence in the COVID-19 vaccine. The programme has seen entire communities go from `the vaccine shot will kill us’ and `women who get vaccinated become infertile’ to ‘the vaccine has helped us re-gain our livelihoods’. Such was the case in the village of Rangaon in Madhya Pradesh, where in the initial phases, only 10% of the population had been inoculated. After continuous efforts, the village has managed to reach 98% vaccination rates. Samhita is working to replicate this success rate in underserved communities across the country.